
Wadia CME March 2014Dr. S. S. Prabhu & Dr. T. H. ManiarDr. Sumitra V. & Dr. Aditi shah

Wadia OSCE March 2014
OSCE 1

DIAGNOSIS
HbF
HbA2
HbA
HbS
A
1-5%
>3.5%
PRESENT
_
B
70-95%
2%
TRACE
_
C
98%
2%
TRACE ORABSENT
_
D
100%
_
_
_
E
_
>90%
F
>3.5%
PRESENT
50%
1.Give diagnosis in each
2.Mention the doses of any (two) chelating agentsused for managing iron overload in thalassemiapatients.
Wadia OSCE March 2014
OSCE 1 / A - ANSWER

DIAGNOSIS
HbF
HbA2
HbA
HbS
THALASSEMIA MINOR
1-5%
>3.5%
PRESENT
_
THALASSEMIAINTERMEDIA
70-95%
2%
TRACE
_
THALLASEMIA MAJOR
98%
2%
TRACE OR ABSENT
_
HERIDITARY PERSISTENCEOF FETAL Hb
100%
_
_
_
SICKLE CELL ANEMIA
_
>90%
HbS/b+ SICKLE THAL
>3.5%
PRESENT
50%
Wadia OSCE March 2014
OSCE 1 /B ANSWER
2.DEFERIPRONE- 75-99 mg/kg/day in 3-4divided doses po
DEFERASIROX -20-30 mg/kg/day OD po
DESFERIOXAMINE-20-40mg/kg/day) SC over8-24 hours using a small portable pump
Wadia OSCE March 2014
OSCE 2
Q1. Mention 2 ECG effects not toxicity of digitalis (Mark 1)
Q2. Match the following(Mark 3)
Prolonged QTc segment- Hypercalcemia
Shortens QTc- Hypokalemia
ST segment depression- Hypocalcemia
Q3. When the QRS complexes are equiphasic in limb leads known as ____________________phenomenon. (Mark1)
Q4. Describe and diagnose the ECG

Wadia OSCE March 2014
Answer 2
Q1. Digitalis effects on ECG are (Mark 1)
Shortening of corrected QT interval
Depression of terminal portion of ST segment
Diminished magnitude of T wave
Q2. Match the following(Mark 3)
Prolonged QTc segment- hypocalcemia
Shortens QTc- Hypokalemia
ST segment depression- hypercalcemia
Q3. .(Mark1 ) When the QRS complexes are equiphasic in limb leads known as ____________________phenomenon.
Q4 . Second degree AV block Mobitz Type 1
•Wenckebach phenomenon
Wadia OSCE March 2014
OSCE 3Mention NORMAL or ABNORMAL in each box

DIAGNOSIS
aPTT
PT
BT
PLATELETES
1
AFIBRINOGENEMIA
2
FACTOR VIII DEF
3
DIC
4
FACTOR XIII DEF
5
BERNARD SOULIER SYN
6
HEPARIN
Wadia OSCE March 2014
ANSWER 3

DIAGNOSIS
aPTT
PT
BT
PLATELETES
1
AFIBRINOGENEMIA
Abn
Abn
Abn
NORMAL
2
FACTOR VIII DEF
Abn
NORMAL
NORMAL
NORMAL
3
DIC
Abn
Abn
Abn
ABNORMAL
4
FACTOR XIII DEF
NORMAL
NORMAL
NORMAL
NORMAL
5
BERNARD SOULIER SYN
NORMAL
NORMAL
Abn
NORMAL
6
HEPARIN
Abn
NORMAL
NORMAL
NORMAL
Wadia OSCE March 2014
OSCE 4
1. What Is This Sign To Check Newborn Maturation?
2. What is the formula for calculation of ponderal index?
3. What is its significance of ponderal index?
4. Mention dose and method of administration of caffeinecitrate in apnea of prematurity.

Wadia OSCE March 2014
ANSWER - 4
1.Scarf sign
2.PI=Weight (gm)/length in cm3
3. Pi<2- asymmetric IUGR
Pi 2-2.5- symmetric IUGR
Pi>2.5 – normal
4. Caffeine is given as a respiratory stimulant in cases of apnea of prematurity.
When given to infants <1250 g in first 10 days of life it decrease
The risk of BPD:
Loading dose: 20mg/kg iv slow over >30 min in infusion pump
Maintenance dose : 5-12 mg/kg iv or PO starting 24 hrs after loading dose
Wadia OSCE March 2014
OSCE 5
5 year old child with h/o recurrent pain in abdomen
And constipation.
Mother noticed that child was very hyperactive and aggressivesince past 2-3 weeks .
H/o dragging of the right leg while walking since 1 Week.
H/o taking ayurvedic medicines since 2 years on their Own.
On examination Pallor was noticed by the referring doctor.
1.What is your clinical suspicion?
2.Name the test to confirm your clinical impression.
3.When will you start treatment?
4.What is the drug of choice?
Wadia OSCE March 2014
OSCE 5 - ANSWER
1.Lead poisoning
2.Blood Lead Level
3.IN all patients with lead encephalopathy,chelation is started.
•Venous blood lead levels >45 mcg/dl shouldbe treated with chelation.
Blood Lead Level:
•45 TO 70= DMSA
•>70 = CaEDTA + BAL or DMSA
Wadia OSCE March 2014
OSCE 6
•An 8 y old child presents with fever off and on andabdominal distension for last 2 months – no othersymptoms
•O/E : average built, child looking unwell
liver ++ firm, not tender
no splenomegaly no ascites
JVP raised, HJR –ve
1.Probable diagnosis ?
2.Mention (any one) clinical differentialdiagnosis
3.Draw JVP wave form with waves for thiscondition
Wadia OSCE March 2014
Answer 6
•An 8 y old child presents with fever off and on and abdominaldistension for last 2 months – no other symptoms
•O/E : average built, child looking unwell
liver ++ firm, not tender
no splenomegaly, no ascites
JVP raised, HJR –ve
•Probable diagnosis ?
•Constrictive pericarditis
•Explanation :
–Congested liver and neck veins – obstruction to superior and inferior venacava– of infective origin
•Mention (any one) clinical differential diagnosis
–Restrictive cardiomyopathy
–Pericardial effusion
•Draw JVP wave form with waves for this condition
–Prominent and Deep ‘y’ descent
–Paradoxical JVP : rises with inspiration and drops with expiration
Wadia OSCE March 2014
osce7
4 yrs old boy brought by parents with complaints fromschool teacher that child has poor concentration, failsto complete the tasks given, keeps moving around inthe class and cannot wait for his turn.
1.What is the possible diagnosis?
2.What screening test will you do in the clinic?
3.What are the criteria for further evaluation?
4.Name any 3 comorbid conditions.
Wadia OSCE March 2014
Osce 7 - answer
1.ADHD
2.VANDERBILT ADHD “Parent Informant” RATING SCALE.
3.For the ADHD screen, a scored 2 or 3
1.inattentive (items 1-9) : 6 out of 9
2.hyperactive-impulsive ADHD (items 10-18) : 6 out of 9
3.And a score of 4 or 5 on any of the Performance items (48-55).
4.Comorbid to ADHD: ( any 3)
1.LD
2.Language
3.Oppositional defiant
4.Conduct
5.Anxiety
6.Depression
Wadia OSCE March 2014
Osce 8
11 yr old boy with h/o recurrent fever episodes since childhood requiringantibiotics comes with on and off pain in abdomen.
His weight is 16kg , Ht- 117cm.
Hb-7.6, creatinine 5.4,
K- 6.2, Na 140, Cl 114,
Phosp -6.2, Ca 9.7,
USG showing small echogenic kidneys with both ureters dilated.
1.What is the likely diagnosis?
2.Calculate e-GFR of this patient.
3.Stage this condition based on GFR.
4.How will you treat anemia?
5.What other test will you do for prognosis ?
Wadia OSCE March 2014
Answer 8
1.Reflux nephropathy with CRF with failure to thrive
2.GFR= k x ht/sr. creatinine
0.7 x 117/5.4 =15.16
3. Stage 4 of chronic kidney disease -severe decrease in GFRSTAGE 1: GFR >90Stage 2: 60-89Stage 3: 30-59Stage 4: 15-29Stage 5: <15or on dialysis4. Inj erythropoietin s.c. :start with 50mcg/ kg/ dose 3 times per week Not on dialysis : dose range of 50-250 mcg/ kg/ dose 3times per week On dialysis : 50-450mcg/ kg/ dose 2-3 times per week5. DMSA to see degree of scarring and function
Wadia OSCE March 2014
OSCE 9
•A 7yr old child admitted with Acute Gastroenteritis withsevere dehydration.
ABG:-
pH 7.15, pCO2- 35mmHg, HCO3 14 mEq/L,
BSL-90
Na+ -140mEq/L
K - 3.5mEq/L
Cl - 110mEq/L
BUN - 15
•What is the ABG diagnosis? (1)
•How you calculate expected PCO2 compensation (1)
•How you calculate osmolatity ? (1)
•What is formula to calculate Oxygenation Index (OI) ? (1)
Wadia OSCE March 2014
Answer 9
•Normal anion gap metabolic and respiratoryacidosis
•ExpectedCo2= HCO3X1.5+8 +/- 2
• = 14X1.5 +8+/- 2= 27-31
•Osmolatity = 2X Na + Glucose/18 + BUN/2.8
• = 2x140 +90/18 +15/2.8
• =280+5+5.35= 290.35
•OI = MAP X FiO2 X 100 /Postductal PaO2
Wadia OSCE March 2014
OSCE 10
A 14 yrs old boy brought in OPD at parental concern .On evaluation he has preadolescent male genitalia,scanty axillary hair and no pubic hair.
1.What is the Tanner staging of this boy? (1)
2.At what Tanner staging Male child attain peakgrowth velocity? (1)
3.At what Tanner staging Female child attainmenarche? (1)
4.Define precocious puberty in male (1)
5.Define precocious puberty in Female (1)
Wadia OSCE March 2014
Answer 10
1.SMR 1
2.SMR 3-4
3.SMR 4
4.Precocious puberty before 8 yrs in girls and
5.Before 9 yrs in male
Wadia OSCE March 2014
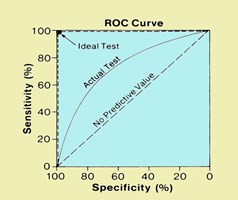
OSCE 11 :
•What is name of curve ? (1)
•What are it’s uses ? (1)
Determine the sample size to find out the Vitamin A requirement in the under fivechildren of Pune district .
From the existing literature the mean daily requirement of the same wasdocumented as 930 I.U with a SD of 90 I.U.
Consider the precision as 9.
Wadia OSCE March 2014
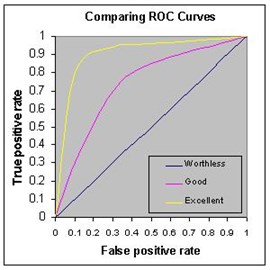
OSCE 11 A
•A receiver operating characteristic (ROC)curve
•ROC analysis provides tools to select possiblyoptimal models and to discard suboptimalones.
Wadia OSCE March 2014
ANSWER 11B
Quantitative data
N = 4SD2/L2
4 x 90 x 90 /9 x9 = 400
•Qualitative data N = 4pq/L2
•P = positive factor /prevalence/proportion
•Q = 100 – p
•L = allowable error or precision or variability
•4 = 1.962(Alpha error) 2
Wadia OSCE March 2014
ANSWER 11B

Condition positive
Condition negative
Testoutcome
Testoutcomepositive
True positive
Testoutcomenegative
True negative
Wadia OSCE March 2014
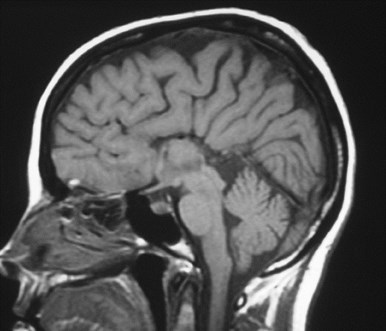
OSCE 12
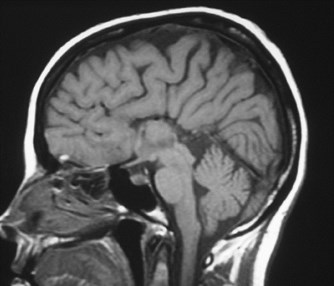
1. Identify and describe the MRI findings.
2.What is probable diagnosis ?
3. Name 2 syndromes In which this feature is seen?
4. What are characteristic clinical presentations?
Wadia OSCE March 2014
Answer 12
1.Sagittal T1-weighted MRI of the brain shows complete absence of the corpus callosum.(1)
2.Corpus callosum agenesis (1)
3.Aicardia Syndorme, Andermann syndrome,Shapiro syndrome, Septooptic dysplasia(1)
4.Vision impariment, Hypotonia, poor muscle coordination, Developmental delay (1)
Wadia OSCE March 2014
OSCE 13

1.Name the organism ?
2.What is the commonest presentation inimmuno-competent children?
3.Name any two conditions where thisorganism causes severe disease?
4.What is the drug of choice by FDA ?
5.Write following journal article in Vancouver style
Article :Cardiogenic Shock With Hypereosinophilic Syndrome
Authors :Vinitha Prasad, L Rajam and Ashwin Borade
Journal : Indian Pediatrics
Year :2009
Volume : 46
Page : 801-803
Wadia OSCE March 2014
Answer 13
•Giardia Lamblia
•Mostly asymptomatic (but rarely Sudden onset explosivewatery diarrhea with distension of abdomen)
•Immunocompromised
–Nephrotic syndrome
–Primary immunodeficiemcy( e.g. CVID)
• Tinidazole ,Nizonide
•Author's surname Initials, Author's surname Initials. Title ofarticle. Title of Journal. [abbreviated] Year of publicationMonth date;Volume Number(Issue number):page numbers.
Prasad V, Rajam L , Borade A. Cardiogenic Shock WithHypereosinophilic Syndrome. Indian Pediatr. 2009;46: 801-3.
Wadia OSCE March 2014
STATION 14
Arrange following food items in
descending order of calories content.
( no need to write the calories)
• 1 cup Tea
•1 TSF Sugar
•1 glass milk ( 200 ml)
•1 cup Cooked Rice
•1 egg
• 1 TSF Ghee/ Butter
•1 TSF cooked dal
Write down the age at whichfollowing reflex appears
a)Palmer grasp
b)Rooting reflex
c)Moro reflex
d)Tonic neck reflex
e)Parachute reflex
Wadia OSCE March 2014
Answer 14 A
•1 cup Cooked Rice 175
•1 glass milk ( 200 ml) 120
•1 egg 80
•1 cup Tea 60
•1 TSF Ghee/ Butter 36
•1 TSF Sugar 20
•1 TSF cooked dal 10
Wadia OSCE March 2014
Answers 14 B
a)Palmer grasp 28 Wks
b)Rooting reflex 32 Wks
c)Moro reflex 28-32 Wks
d)Tonic neck reflex 35 Wks
e)Parachute reflex 7-8 months
Wadia OSCE March 2014
STATION 15Match the following antidotes
a)Paracetamol Atropine/PAM
b)Dhatura BAL
c)Cyanide myl Nitrite
d)Mercury Physostigmine
e)OP N- Acetylcysteine
f)INH Naloxone hydrochloride
g)Opiods Pyridoxine
Wadia OSCE March 2014
Answers 15
a)Paracetamol N- Acetylcysteine
b)Dhatura Physostigmine
c)Cyanide Amyl Nitrite
d)Mercury BAL
e)OP Atropine/PAM
f)INH Pyridoxine
g)Opiods Naloxone hydrochloride
Wadia OSCE March 2014
OSCE 16
1.Give five radiologicalfindings ?
2.What is the diagnosis ?
3.What is the management ?

Wadia OSCE March 2014
Answer 16
1. Ground glass appearance of bone2
2. Thinned cortex
3. Periosteal calcification
4. White line of Fraenkel (well calcified cartilage)
5. Wimberger’s sign (white ring)
Diagnosis : Scurvy 1
Treatment :
1. Vit. C 100-200 mg/ day1
2. Dietary Therapy
Total 4 marks
Wadia OSCE March 2014
OSCE 17
1.Identify the test done in picture? ( 1 )
2.What is indication for procedure? (1)
3.What is the diagnosis? (1)
4.What dye is used ? (1)
5.What is the treatment of choice?(1)

@24 hours
Wadia OSCE March 2014
Answer 17
1.Hepatobiliary Scintigraphy
2.Neonatal Cholestasis
3.No bowel activity can be seen. Delayed images at 24hours demonstrated persistent hepatic activity, nobowel activity, S/O biliary atresia
4.Radioactive dye Tc HydroxyIminoDiaetic Acid (HIDA)
5.Kasai procedure before 8 wks of life
24 hours
Wadia OSCE March 2014
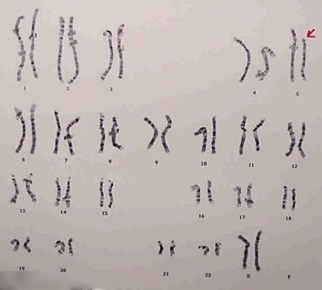
•What is the diagnosis
•What is the defect
•What is commonest presentation ?
•What cardiac lesion can be seen with this?
•What facial feature can be seen with this?
OSCE 18Neonate with acharacteristic cryhad thisKaryotype …
Wadia OSCE March 2014
Answer -18
•Cri Du Chat syndrome
•Micro deletion of short arm of chr, 5
•Cat like cry ( hypotonic, SS, microcephaly)
•VSD, ASD,PDA ( septal defects)
•Microcephaly, moon like face, hypertelorisum,epicantal fold, wide flat nasal bridge
Wadia OSCE March 2014
OSCE 19

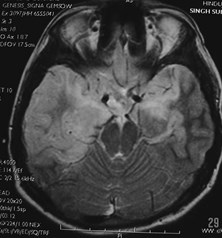
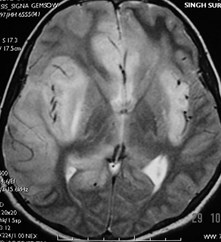
Interpret the MRI (1)
Interpret the EEG (1)
What is the mostprobable diagnosis (1)
Name the drug of choice(1)
What is the definition ofEosinophilic Meningitis(1)
Wadia OSCE March 2014
Answer 19
•Cortical damage seen in Bilateral temporallobes
•PLEDS Periodic lateralizing EpileptiformDischarges
•HSV Encephalitis
•Acyclovir
•10 or more eosinophils/mm3of CSF
Wadia OSCE March 2014
OSCE 20Watch the video and answer thefollowing questions.
•Describe the Gait.
•Give clinical diagnosis with probableanatomical location of the lesion.
Wadia OSCE March 2014
Answer 20Watch the video and answer thefollowing questions.
•Describe the Gait.
–Right LL Circumduction gait
–Internally rotated Rt. foot
–Poor Rt UL movement
–Flexion at elbow
–Thumb adducted Rt Hand
•Give clinical diagnosis with probable anatomical location of the lesion.
–Right Hemiparesis.
–Left internal capsule or corona radiata
(Facial may have improved)
Wadia OSCE March 2014
OSCE 21 -A
•Counsel parents of a 1 year old child withsecond episode of febrile seizure
Wadia OSCE March 2014
ANSWER 21- ACounsel parents of a 1 year old child with second episode offebrile seizure
•Introduction
•Diff bet simple & atypical FS
•FH/o FS
•Developmental history
•Explains-
1.Common
2.First aid during episode
3.Treatment options-intermittent/cont prophylaxis
•Questions: need for inv/dev of her child/recurrence in sibs
•Add common at this age ( 5-7%)
•Reassurance about good prognosis and normal development
•Recurrence during further episodes but disappearce usually after 5-6 years
•No major investigations required unless repeated episode or atypical features
•Need for antipyretics / anti-inflammatory during episode
Wadia OSCE March 2014
OSCE 21 - BCounsel the mother, whose child hasbeing diagnosed with Haemophilia A
Wadia OSCE March 2014
ANSWER 21 BCounsel the mother, whose child has being diagnosed with Haemophilia A

Introduction
½
Explain the disease
½
Removal of guilt
½
Problem addressed – current problems (Jt. Bleed ))
½
Associated problems.. deep bleeds
½
Treatment drug / dosage / side effect to watch Factor VIII / Cryo / FFP
1
On discharge : precautions at home
½
Precautions at school / play . Helmet / knee / elbow
½
To inform about the condition in case of any future medical intervention
½
Counsel for future preg / posibility of pre natal diagnosis for her and others inFamily
1
Investigate other RELEVENT members
½
School / play
½
Future cure / vaccination MAY come up …
½
When to follow up
½
When to come in emergency?
½
Ask if they have any more questions?
½
Thank the Mother
½
TOTAL
10
Wadia OSCE March 2014
OSCE 21 - C
•Counsel the mother of a 8 yr old boy, who isdiagnosed to have mild persistent asthmaabout inhaler therapy.
Wadia OSCE March 2014
Answer – 21 - C
1.Introduces / language
2.Explains about basic pathology – simple terms
3.Myths about inhalers
4.Chooses correct inhaler ( preventer & reliever)
5.Spacer
6.Demonstrates how to use
7.To Rinse mouth after use
8.How to clean spacer
9.How to check empty
10.How to monitor : Peak Flow Meter / cough diary
11.When to follow up
12.When to come early ( emergency)
13.Asks any more Questions??
14.Says Thank you
Wadia OSCE March 2014
OSCE 22
•REST Station
Wadia OSCE March 2014
OSCE 23- A
•Take relevant history of 2 yr old child broughtby parents with c/o speech delay
Wadia OSCE March 2014
Answer 23 A
•Introduction ,establish rapport 1
•Detail speech development history1
•Other developmental delay-gross motor, fine motor, adaptive/ social 1
•Birth/H- preterm,NICU,congenital infections 1
•F/H/O- global DD, MR, deafness 1
•H/O hearing defect, neonatal meningitis (1)
•Socioeconomic and social opportunity given or not (1/2)
•Facial/local anomalies- tongue tie ½
•Autism- mixing with friends, social contact ½
•Thanking ½
Wadia OSCE March 2014
OSCE – 23 - B
•HISTORY TAKING
•4 year old male child brought to you with
•H/o limping left leg acute onset take history.
Wadia OSCE March 2014
Answer : 23 – BHISTORY TAKING
1.Introduces/Explains
2.Problems
3.Which limb – joint
4.Swelling of the joint/redness/tenderness
5.Onset, Duration/progression
6.Fever/constitutional symptoms/wt loss/rash
7.Restriction of movements
8.H/o trauma
9.H/o vaccination/injection
10.Other limbs/joints
11. Cardiac symptoms
12.H/o Koch’s contact
13.H/o Gastro/sickle/haemophilia/ HSP
14.Thank you
Wadia OSCE March 2014
OSCE 24
•REST Station
Wadia OSCE March 2014
OSCE 11
•What is VISION 2020?
•When it was launched?
•Who initiated this program?
•AT National level who participate in it?
Wadia OSCE March 2014
Answer 11
•VISION 2020 is the global initiative for theelimination of avoidable blindness.
•It was launched in 1999.
•jointly by the World Health Organization(WHO) and the International Agency for thePrevention of Blindness (IAPB).
•At the national level, a strong partnershipbetween Ministry of Health, national andinternational NGOs, professional organizations,and civil society groups.
Wadia OSCE March 2014
ELICITING KNEE JERK
Greeting the patient and self introduction
Taking consent and explaining the procedure.
Adequate exposure
Proper position of the patient (supine) and the doctor
Holding hammer properly and striking sweep with elbow
Proper technique (Keeping the hand under the knee andstriking the patellar tendon midway between its originand insertion).
Looking for quadriceps contraction.
Grading the reflex
Thanking the patient.
Wadia OSCE March 2014
Wish You All The Best !
Wadia OSCE March 2014